Overview
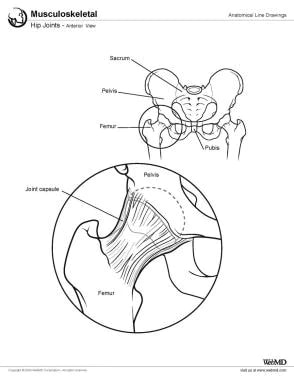
The hip joint (see the image below) is a ball-and-socket synovial joint; the ball is the femoral head, and the socket is the acetabulum. The hip joint is the articulation of the pelvis with the femur, which connects the axial skeleton with the lower extremity. The adult os coxae, or hip bone, is formed by the fusion of the ilium, the ischium, and the pubis, which occurs by the end of the teenage years. The two hip bones form the bony pelvis, along with the sacrum and the coccyx, and are united anteriorly by the pubic symphysis. This joint is essential for both mobility and stability, allowing for a wide range of movements while supporting body weight. [1]
Gross Anatomy
Bones and osteology
Femur
The femur is the longest and heaviest bone in the human body. It consists of a superior or proximal end, a shaft, and an inferior or distal end (see the image below). The greater trochanter of the femur is a crucial landmark to guide surgeons during anterolateral approaches to the hip joint. It can be palpated on the upper part of the lateral thigh, inferior to the midpoint of the iliac crest and approximately level with the horizontal plane passing through the pubic tubercle. [1]

The superior end of the bone is the articulating side of the femur to the acetabulum. The upper femoral epiphysis closes by 16 years of age.
The trabecular bone configuration in the proximal femur obeys Wolff's law, which states that bony structures orient themselves in form and mass so as to best resist extrinsic forces. The principal compressive group, the principal tensile group, the greater trochanteric group, the secondary tensile group, the secondary compressive group, and, finally, Ward's triangle can be found.
The superior end of the femur consists of a head, a neck, and greater and lesser trochanters. The head of the femur is angled superomedially and slightly anteriorly when articulating with the acetabulum. The head is attached to the femoral body or shaft by the neck of the femur.
The superior border of the neck begins just lateral to the femoral head and ends distally at the greater trochanter. The inferior border of the neck begins lateral to the femoral head and extends to the inferior trochanter. The superior border is shorter and thicker than the inferior border. The anterior surface of the neck is rough in comparison to the smooth femoral head. The neck's posterior surface has a concave appearance. The head and neck are at an angle of 130° (± 7°) to the shaft. The angle is larger at birth and decreases with age.
The greater trochanter is a bony prominence on the anterolateral surface of the proximal shaft of the femur, distal to the femoral neck. It serves as the insertion site for the gluteus medius and gluteus minimus. The lesser trochanter is a bony prominence on the proximal medial aspect of the femoral shaft, just distal to the femoral neck. It serves as the iliopsoas insertion site.
The intertrochanteric line is a raised area that extends from the greater to the lesser trochanter anteriorly. This connection posteriorly is called the intertrochanteric crest, which contains the calcar femorale, another anatomic location on the femoral neck. The calcar femorale is a vertically oriented plate of dense cancellous bone from the posteromedial portion of the femoral shaft radiating superiorly toward the greater trochanter. [2]
Studies indicate that the vertical head diameter averages 40.89 ± 4.26 mm, with a neck-shaft angle typically ranging from 125° to 135°, decreasing with age. The intertrochanteric distance averages 53.67 ± 7.19 mm, reflecting differences in skeletal morphology between individuals and across populations. [3]
Pelvis
At birth, each pelvic half consists of three separate primary bones: the ilium, the ischium, and the pubis (see the images below). These bones are joined by hyaline cartilage.


In infants and children, these large parts of the hip bones are incompletely ossified. At puberty, the three primary bones are still separated by a Y-shaped triradiate cartilage centered in the acetabulum. The primary bones begin to fuse at 15-17 years of age. Fusion is complete between 20 and 25 years of age. The fact that these bones were originally separate is fairly undetectable in adult bones on imaging. Although the parts of the hip bone are fused in adulthood, they are still referred to by their separate origins. [4]
Anatomical landmarks such as the iliac crest, ischial tuberosity, and pubic symphysis are critical attachment sites for muscles and ligaments and play key roles in pelvic stability and lower limb movement. The acetabulum, formed from portions of all three bones, serves as the articulation site for the femoral head, creating the hip joint's ball-and-socket structure essential for a wide range of motion. [1]
Ilium
The ilium is the largest part of the hip bone and makes up the superior part of the acetabulum. Structurally, the ilium is divided into two main parts: the ala (wing) and the body. The ala is the broad, fan-shaped portion that expands superiorly, while the body contributes to the acetabulum and provides a site of articulation with the ischium and pubis. [1]
The ala provides an insertion point for the gluteal muscles laterally and the iliacus muscle medially.
Anteriorly, the ilium has an anterior superior iliac spine (ASIS). This prominent projection serves as a crucial landmark for various anatomical measurements and is an attachment point for the inguinal ligament and sartorius muscle. [1] Inferior to this is an anterior inferior iliac spine that serves as an attachment site for the rectus femoris muscle and iliofemoral ligament. [1]
From the ASIS, anteriorly, the iliac crest comes around laterally and continues posterior to the posterior superior iliac spine (PSIS). The PSIS marks the superior point of the greater sciatic notch. The iliac crest is a significant landmark and serves as an attachment site for abdominal and back muscles. [1]
The lateral surface of the ilium has three rough curved lines: the posterior, anterior, and inferior gluteal lines. Medially, the ilium has an iliac fossa, which serves as an attachment site for the iliacus muscle. [1] Posteriorly, the medial aspect of the ilium has an auricular surface. [4] This surface articulates with the sacrum to form part of the sacroiliac joint. [1]
Studies have provided detailed insights into the developmental anatomy of the ilium, focusing on its primary ossification center. The primary ossification center of the ilium begins forming during fetal development, typically around the 9th week post-fertilization. A study analyzed its growth dynamics in fetuses aged 18-30 weeks, with crown-rump lengths (CRL) ranging from 130 to 265 mm. The growth of the ossification center has been evaluated in terms of its linear (vertical and transverse diameters), planar (projection surface area), and volumetric parameters. [5]
Linear parameters: [5]
-
The vertical diameter of the ossification center increases logarithmically, following the function y = −63.138 + 33.413 × ln(CRL) ± 1.609
-
The transverse diameter also grows logarithmically as y = − 59.220 + 31.353 × ln(CRL) ± 1.736
These patterns indicate a consistent and predictable growth pattern during fetal development.
Planar and volumetric parameters: [5]
-
The projection surface area increases linearly with CRL, described by y = − 105.681 + 1.137 × CRL ± 16.035
-
Similarly, the volume of the ossification center follows a linear growth model; y = 478.588 + 4.035 × CRL ± 14.332
Throughout the study period, the shape of the ilium's primary ossification center remained stable, as evidenced by a constant transverse-to-vertical diameter ratio of approximately 0.94 ± 0.07. This stability suggests that while the size increases, the overall shape does not change significantly during this stage of development. [5]
The study found no significant differences in size or growth dynamics between sexes or between the right and left sides of the ilium's ossification centers. This uniformity allows for standardized reference data to be used in prenatal diagnostics. Understanding these developmental dynamics is crucial for assessing fetal maturity and identifying congenital disorders. [5]
Ischium
The ischium is the inferior aspect of the pelvis. The superior part of the body of the ischium fuses with the pubis and ilium, forming the posteroinferior aspect of the acetabulum.
The body of the ischium contributes to forming approximately two-fifths of the acetabulum. The external surface contributes to the acetabular fossa, while internally, it forms part of the lesser pelvis. [1]
The ramus of the ischium joins the inferior ramus of the pubis to form a bar of bone called the ischiopubic ramus, which constitutes the inferomedial boundary of the obturator foramen. The posterior border of the ischium forms the lower margin of a deep indentation, the greater sciatic notch. The large triangular ischial spine at the inferior margin of this notch is a sharp demarcation separating the greater sciatic notch from a smaller rounded inferior indentation called the lesser sciatic notch.
The bony projection at the inferior end of the body of the ischium and its ramus is the ischial tuberosity. [4] It provides attachment sites for muscles such as the hamstrings and adductor magnus. [1]
Pubis
The pubis makes up the anteromedial part of the hip bone and contributes to the anterior part of the acetabulum. The pubis has a flat body and two rami: superior and inferior.
Medially, the symphyseal surface of the body of the pubis articulates at the pubic symphysis with the surface of the body of the contralateral pubis. This joint is a nonsynovial amphiarthrodial joint, stabilized by a fibrocartilaginous disc sandwiched between thin layers of hyaline cartilage. [6]
The anterosuperior border of the united bodies and symphysis forms the pubic crest. The pubic tubercles, small projections at the lateral ends of this crest where the inguinal ligaments attach medially, are extremely important landmarks of the inguinal regions.
The posterosuperior aspect of the superior ramus of the pubis is called the pectin pubis or pectineal line. This ridge provides attachment for part of the pectineus muscle and contributes to the pelvic brim. [1]
The obturator foramen is an oval opening formed by the rami of the pubis and the ischium. The obturator canal houses the obturator nerve and vessels. [4]
The pubis serves as an attachment site for several muscles, including: [1]
-
Rectus abdominis
-
Pectineus
-
Adductor muscles of the thigh (adductor longus, brevis, magnus)
-
Gracilis
-
Pubococcygeus muscle (part of the pelvic floor)
The pubic symphysis allows limited movement (up to 2 mm shift and 1° rotation) under normal conditions but becomes more mobile during pregnancy due to hormonal influences, such as those caused by relaxin. [7]
Acetabulum
As indicated above, the acetabulum is formed from parts of the ilium, ischium, and pubis. The acetabulum is the cup-shaped socket on the lateral aspect of the pelvis, which articulates with the head of the femur to form the hip joint.
The margin of the acetabulum is deficient inferiorly. An additional fibrocartilaginous margin of the acetabulum is referred to as the acetabular labrum. The labrum functions to deepen the acetabulum, thus holding the femoral head more securely. The lunate is the articular surface of the acetabulum to the femoral head. The rough depression in the floor of the acetabulum is the acetabular fossa, which is continuous with the acetabular notch.
The transverse acetabular ligament is located along the inferior aspect of the acetabulum; it prevents the femoral head from moving inferiorly by deepening the acetabulum inferiorly.
Studies have provided detailed morphometric data on acetabular dimensions. The average diameter and depth of the acetabulum have been reported as approximately 48-49 mm and 23-25 mm, respectively. [8]
Ligaments
The hip joint contains a strong fibrous capsule that attaches proximally to the acetabulum and transverse acetabular ligament and distally to the neck of the femur, anteriorly at the greater trochanter (see the image below). Posteriorly, the fibrous capsule crosses to the neck 1-1.5 cm proximal to the intertrochanteric crest.

Most of the fibers go from the hip bone to the intertrochanteric line, but some deeper fibers go around the neck, forming the orbicular zone, which holds the femoral neck in the acetabulum. The anterior capsule of the hip is the strongest and thickest part.
This capsule is composed of three ligaments. The iliofemoral ligament, sometimes referred to as the Y ligament of Bigelow, attaches to the anterior inferior iliac spine and the acetabular rim proximally and takes an inferolateral direction to insert on the intertrochanteric line distally. It is the strongest part of the capsule. It plays a crucial role in stabilizing the hip joint by limiting external rotation in flexion and both internal and external rotation in extension. [9] The iliofemoral ligament prevents hyperextension of the hip joint during standing by holding the femoral head within the acetabulum. Injuries to this ligament can lead to persistent anterior capsule defects, resulting in hip instability. [9]
The ischiofemoral ligament reinforces the capsule posteriorly. It originates on the ischial part of the acetabular rim and spirals superolaterally to the neck of the femur, medial to the greater trochanter. This ligament, like the iliofemoral, also prevents hyperextension and holds the femoral head within the acetabulum. The ischiofemoral ligament's role in posterior stabilization is crucial for maintaining hip joint integrity. [1]
The pubofemoral ligament reinforces the capsule anteriorly and inferiorly. It begins from the obturator crest of the pubic bone and passes inferolaterally to join the fibrous capsule of the hip joint. The ligament prevents overabduction of the hip joint. [4]
An iliopectineal bursa lies anteriorly over the gap in the ligaments, beneath the iliopsoas tendon.
There are several additional structures of importance related to the fibrous capsule. Lining the fibrous capsule is the synovial membrane. It covers the neck of the femur between the attachment of the fibrous capsule and the edge of the articular cartilage of the head; it also covers the nonarticular area of the acetabulum, providing a covering for the ligament of the femoral head.
Retinacula, which contain blood vessels, are deep longitudinal fibers of the capsule that go superiorly from the femoral neck and blend with the periosteum. The bursa is considered the synovial extension beyond the free margin of the fibrous capsule onto the posterior aspect of the femoral neck.
The ligament of the femoral head is weak. It attaches to the margins of the acetabular notch and the transverse acetabular ligament; its narrow end attaches to the pit in the head of the femur. Usually, the ligament contains a small artery to the head of the femur. [4]
A fat pad in the acetabular fossa is covered with a synovial membrane. It fills the acetabular area that is not filled by the femoral head.
Nerve supply
The nerve supply to the hip joint is outlined in Table 1 and the images below. [10]
Table 1. Nerves of the Hip Joint (Open Table in a new window)
Nerve |
Root Level |
Sensory |
Motor |
Genitofemoral |
L1-2 |
Proximal anteromedial thigh |
None in hip and thigh |
Obturator |
L2-4 |
Inferomedial thigh |
Gracilis (anterior division) Adductor longus (anterior division) Adductor brevis (anterior/posterior division) Adductor magnus (posterior division) |
Lateral femoral cutaneous |
L2-3 |
Lateral thigh |
None |
Femoral |
L2-4 |
Anteromedial thigh |
Psoas major Sartorius Articularis genus Rectus femoris Vastus lateralis Vastus intermedius Vastus medialis |
Tibial |
L4-S3 |
None in thigh |
Biceps femoris (long head) Semitendinosus Semimembranosus |
Common fibular (peroneal) |
L4-S2 |
None in thigh |
Biceps femoris (short head) |
Posterior femoral cutaneous nerve |
S1-3 |
Posterior thigh |
None |
| Superior gluteal nerve [1] | L4-S1 | Superior portion of hip capsule | Gluteus medius, gluteus minimus, tensor fasciae latae |
| Inferior gluteal nerve [1] | L5-S2 | Limited sensory contribution to posterior capsule | Gluteus maximus |
| Nerve to quadratus femoris [1] | L4-S1 | Posterior and inferior portions of hip capsule; ischiofemoral ligament | Quadratus femoris, inferior gemellus |


Musculature
The muscles of the hip joint are outlined in Table 2 and the images below. [10]
Table 2. Muscles of the Hip Joint (Open Table in a new window)
Muscle |
Action |
Nerve |
Sartorius |
Hip flexion, external rotation |
Femoral nerve |
Iliopsoas |
Hip flexion |
Femoral nerve |
Pectineus |
Hip flexion |
Femoral nerve |
Rectus femoris |
Hip flexion, leg extension |
Femoral nerve |
Adductor magnus (anterior part) |
Hip flexion, adduction |
Obturator |
Adductor magnus (posterior part) |
Thigh extension |
Tibial |
Gracilis |
Hip flexion, adduction, internal rotation |
Obturator |
Tensor fascia lata |
Hip flexion, abduction |
Superior gluteal nerve |
Adductor brevis |
Hip adduction |
Obturator nerve (posterior division) |
Adductor longus |
Hip adduction |
Obturator nerve (anterior division) |
Pectineus |
Hip adduction, flexion |
Femoral |
Obturator externus |
Thigh external rotation |
Obturator nerve posterior division |
Gluteus maximus |
Lateral rotation, extension |
Inferior gluteal nerve |
Piriformis |
Lateral rotation |
Nerve to piriformis |
Obturator internus |
Lateral rotation |
Nerve to obturator internus |
Gemellus superior |
Lateral rotation |
Nerve to obturator internus |
Gemellus inferior |
Lateral rotation |
Nerve to quadratus femoris |
Quadratus femoris |
Lateral rotation |
Nerve to quadratus femoris |
Gluteus medius |
Hip abduction |
Superior gluteal nerve |
Gluteus minimus |
Hip abduction |
Superior gluteal nerve |
Semimembranosus |
Thigh extension, leg flexion |
Tibial |
Semitendinosus |
Thigh extension, leg flexion |
Tibial |
Biceps femoris, long head |
Thigh extension, leg flexion |
Tibial |
Biceps femoris, short head |
Thigh extension, leg flexion |
Common fibular |
The pectineus muscle is primarily innervated by the femoral nerve but may also occasionally receive input from the obturator nerve. [11]

Vasculature
The arteries of the hip are outlined in Table 3 and the image below. [10]
Table 3. Arteries of the Hip Joint (Open Table in a new window)
Artery |
Branches |
Obturator |
Anterior and posterior branches |
Femoral |
In femoral triangle, runs in medial thigh between vastus medialis and adductor longus, in adductor canal, through adductor hiatus, then becomes popliteal artery behind knee Superficial circumflex iliac Superficial epigastric Superficial external pudendal Deep external pudendal Deep femoral artery Descending genicular artery Articular branch Saphenous branch |
Deep femoral artery |
Medial circumflex femoral: major supply to femoral neck and head Lateral circumflex femoral: also supplies femoral neck Ascending branch Transverse branch Descending branch Perforators/muscular branches |
Artery |
Course |
Obturator Artery of ligament teres |
Runs through ligament of femoral head |
Deep femoral artery Medial circumflex femoral Ascending branch Descending branch Lateral circumflex femoral Ascending branch Cervical branches Retinacular arteries Transverse branch Descending branch |
Branches from femoral artery in femoral triangle Between pectineus and iliopsoas to posterior femoral neck Runs on quadratus femoris deep to sartorius and rectus femoris to greater trochanter anteriorly Extracapsular branches of anastomosis Intracapsular branches - run along neck, enter bone at base of femoral head Extends laterally Under rectus femoris |
| Superior gluteal artery [1] | Supplies the gluteal region and forms anastomoses with femoral circumflex arteries |
| Inferior gluteal artery [1] | Supplies the posterior hip joint and proximal thigh; participates in collateral circulation |
| Artery of ligamentum teres [1] | Arises from the obturator artery; important for femoral head blood supply in children |

-
Hip joints, anterior view.
-
Parts of femur.
-
Hip ligaments.
-
Hip nerves, lateral view.
-
Hip nerves, anterior view.
-
Vascular anatomy of hip.
-
Pelvis and acetabulum, with muscle attachment sites.
-
Parts of pelvis.
-
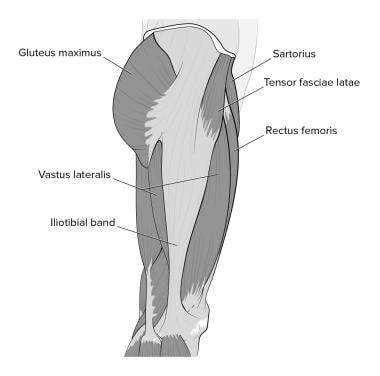
Hip muscles, lateral view.
-
Hip muscles, anterior view.
Tables
Nerve |
Root Level |
Sensory |
Motor |
Genitofemoral |
L1-2 |
Proximal anteromedial thigh |
None in hip and thigh |
Obturator |
L2-4 |
Inferomedial thigh |
Gracilis (anterior division) Adductor longus (anterior division) Adductor brevis (anterior/posterior division) Adductor magnus (posterior division) |
Lateral femoral cutaneous |
L2-3 |
Lateral thigh |
None |
Femoral |
L2-4 |
Anteromedial thigh |
Psoas major Sartorius Articularis genus Rectus femoris Vastus lateralis Vastus intermedius Vastus medialis |
Tibial |
L4-S3 |
None in thigh |
Biceps femoris (long head) Semitendinosus Semimembranosus |
Common fibular (peroneal) |
L4-S2 |
None in thigh |
Biceps femoris (short head) |
Posterior femoral cutaneous nerve |
S1-3 |
Posterior thigh |
None |
| Superior gluteal nerve [1] | L4-S1 | Superior portion of hip capsule | Gluteus medius, gluteus minimus, tensor fasciae latae |
| Inferior gluteal nerve [1] | L5-S2 | Limited sensory contribution to posterior capsule | Gluteus maximus |
| Nerve to quadratus femoris [1] | L4-S1 | Posterior and inferior portions of hip capsule; ischiofemoral ligament | Quadratus femoris, inferior gemellus |
Muscle |
Action |
Nerve |
Sartorius |
Hip flexion, external rotation |
Femoral nerve |
Iliopsoas |
Hip flexion |
Femoral nerve |
Pectineus |
Hip flexion |
Femoral nerve |
Rectus femoris |
Hip flexion, leg extension |
Femoral nerve |
Adductor magnus (anterior part) |
Hip flexion, adduction |
Obturator |
Adductor magnus (posterior part) |
Thigh extension |
Tibial |
Gracilis |
Hip flexion, adduction, internal rotation |
Obturator |
Tensor fascia lata |
Hip flexion, abduction |
Superior gluteal nerve |
Adductor brevis |
Hip adduction |
Obturator nerve (posterior division) |
Adductor longus |
Hip adduction |
Obturator nerve (anterior division) |
Pectineus |
Hip adduction, flexion |
Femoral |
Obturator externus |
Thigh external rotation |
Obturator nerve posterior division |
Gluteus maximus |
Lateral rotation, extension |
Inferior gluteal nerve |
Piriformis |
Lateral rotation |
Nerve to piriformis |
Obturator internus |
Lateral rotation |
Nerve to obturator internus |
Gemellus superior |
Lateral rotation |
Nerve to obturator internus |
Gemellus inferior |
Lateral rotation |
Nerve to quadratus femoris |
Quadratus femoris |
Lateral rotation |
Nerve to quadratus femoris |
Gluteus medius |
Hip abduction |
Superior gluteal nerve |
Gluteus minimus |
Hip abduction |
Superior gluteal nerve |
Semimembranosus |
Thigh extension, leg flexion |
Tibial |
Semitendinosus |
Thigh extension, leg flexion |
Tibial |
Biceps femoris, long head |
Thigh extension, leg flexion |
Tibial |
Biceps femoris, short head |
Thigh extension, leg flexion |
Common fibular |
Artery |
Branches |
Obturator |
Anterior and posterior branches |
Femoral |
In femoral triangle, runs in medial thigh between vastus medialis and adductor longus, in adductor canal, through adductor hiatus, then becomes popliteal artery behind knee Superficial circumflex iliac Superficial epigastric Superficial external pudendal Deep external pudendal Deep femoral artery Descending genicular artery Articular branch Saphenous branch |
Deep femoral artery |
Medial circumflex femoral: major supply to femoral neck and head Lateral circumflex femoral: also supplies femoral neck Ascending branch Transverse branch Descending branch Perforators/muscular branches |
Artery |
Course |
Obturator Artery of ligament teres |
Runs through ligament of femoral head |
Deep femoral artery Medial circumflex femoral Ascending branch Descending branch Lateral circumflex femoral Ascending branch Cervical branches Retinacular arteries Transverse branch Descending branch |
Branches from femoral artery in femoral triangle Between pectineus and iliopsoas to posterior femoral neck Runs on quadratus femoris deep to sartorius and rectus femoris to greater trochanter anteriorly Extracapsular branches of anastomosis Intracapsular branches - run along neck, enter bone at base of femoral head Extends laterally Under rectus femoris |
| Superior gluteal artery [1] | Supplies the gluteal region and forms anastomoses with femoral circumflex arteries |
| Inferior gluteal artery [1] | Supplies the posterior hip joint and proximal thigh; participates in collateral circulation |
| Artery of ligamentum teres [1] | Arises from the obturator artery; important for femoral head blood supply in children |




